

INTRODUCTION: Tocilizumab (toci) is often used to manage cytokine release syndrome (CRS) associated with chimeric antigen receptor T-cell (CAR-T) and T-cell engager (TCE) therapies, including therapies targeting B-cell maturation antigen (BCMA) in relapsed/refractory multiple myeloma (RRMM). Whether CRS development or early time-to-toci (defined as initial tocilizumab within 12 hours of CRS onset) impact 30-day outcomes is unknown. We performed a retrospective analysis of adult RRMM patients at our institution who received anti-BCMA CAR-T or TCE therapy.
METHODS: We reviewed all RRMM patients who received CAR-T/TCE therapy between 7/1/2017 and 6/30/2020. Time-to-CRS was defined as the first temperature ≥ 38°C without clear alternate etiology. CRS resolution was defined as the first timepoint marking defervescence lasting ≥ 24 hours or hospital discharge, whichever was sooner. For patients who developed CRS, we recorded initial and peak CRS grades using consensus criteria (Lee 2019), relevant biomarkers, time of first toci administration, and usage of corticosteroids/anakinra. We also recorded neurotoxicity, persistent neutropenia, and macrophage activation syndrome (MAS)-like features. Patients were categorized into three groups: no toci, early time-to-toci (first dose ≤ 12 hours of CRS onset), and late time-to-toci (first dose > 12 hours of CRS onset). We used logistic regression to predict objective response (≥ partial response [PR] at 30 days, IMWG criteria) and linear regression to predict CRS duration, with covariates including CAR-T/TCE product identity, time-to-CRS, and time-to-toci.
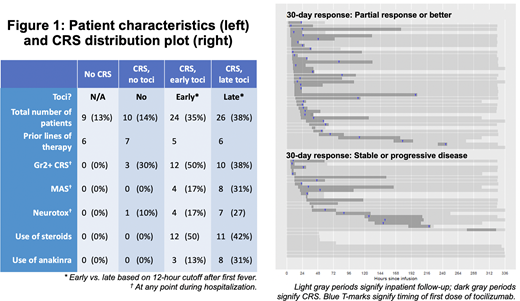
RESULTS: Of the 70 RRMM patients, 14 (20%) received TCE therapy and 56 (80%) received CAR-T therapies; 60 (87%) experienced CRS and 50 (72%) received toci (Figure 1). Of note, 24 patients also received dexamethasone and 11 patients received anakinra while hospitalized. Development of CRS was strongly associated with achievement of ≥ PR by Day 30 (odds ratio [OR] 13.8, 95% confidence interval [CI] 1.6-118). Patients who achieved a ≥ PR at Day 30 had shorter time-to-CRS intervals compared to non-responders (median 11.4 vs 26 hours, p=0.03). Among patients who developed CRS, time-to-CRS <24 hours was associated with achieving ≥ PR by Day 30 (OR 5.76, 95% CI 2.0-16.5).
Of the 50 patients who received toci, 24 (48%) had early time-to-toci (≤ 12 hours) while 26 (52%) had late time-to-toci. Thirty-day response rates were similar between groups (71% early vs 69% late, p=1.0). Among the 48 patients with CRS lasting > 12 hours, receiving toci within 12 hours of CRS onset was associated with shorter total CRS duration (median 45 hours vs 56 hours, p=0.04). Patients who developed MAS-like features and/or neurotoxicity had somewhat lower time-to-toci intervals compared to patients who developed neither (MAS patients median time-to-toci 11.8 hours vs 16.9 hours, p = 0.59; neurotoxicity patients time to toci 12 hours vs 18.3 hours, p=0.15); however, these differences were not significant.
CONCLUSION: In RRMM patients receiving CAR-T/TCE therapy, the development of CRS is associated with achieving ≥ PR at Day 30. Furthermore, responders develop CRS earlier than non-responders. Among patients who develop CRS, early time-to-toci is associated with proportionately shorter CRS duration and does not appear to affect short-term responses, or development of MAS or neurotoxicity. Limitations of our analysis include its retrospective nature with heterogeneity between products and provider decision-making. Our results suggest that early time-to-toci may shorten CRS duration and potentially length of hospitalization. These hypothesis-generating findings warrant validation with longer follow-up. Additionally, prospective protocols implementing early or pre-emptive toci administration, similar to a published approach in lymphoma patients (Gardner 2019), warrant consideration in the RRMM population as well.
Wolf:Adaptive: Consultancy, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau. Martin:Seattle Genetics: Research Funding; AMGEN: Research Funding; GSK: Consultancy; Sanofi: Research Funding; Janssen: Research Funding. Wong:Janssen: Research Funding; Amgen: Consultancy; Bristol Myers Squibb: Research Funding; Roche: Research Funding; GSK: Research Funding; Sanofi: Membership on an entity's Board of Directors or advisory committees; Fortis: Research Funding. Shah:BMS, Janssen, Bluebird Bio, Sutro Biopharma, Teneobio, Poseida, Nektar: Research Funding; GSK, Amgen, Indapta Therapeutics, Sanofi, BMS, CareDx, Kite, Karyopharm: Consultancy.
tocilizumab is an IL-6 receptor antagonist that is currently indicated and FDA approved for: Rheumatoid Arthritis (RA) Adult patients with moderately to severely active rheumatoid arthritis who have had an inadequate response to one or more Disease- Modifying Anti-Rheumatic Drugs (DMARDs). Giant Cell Arteritis (GCA) Adult patients with giant cell arteritis. Polyarticular Juvenile Idiopathic Arthritis (PJIA) Patients 2 years of age and older with active polyarticular juvenile idiopathic arthritis. Systemic Juvenile Idiopathic Arthritis (SJIA) Patients 2 years of age and older with active systemic juvenile idiopathic arthritis. Cytokine Release Syndrome (CRS) Adults and pediatric patients 2 years of age and older with chimeric antigen receptor (CAR) T cell-induced severe or life-threatening cytokine release syndrome.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal